

Introduction
Progressive multifocal leukoencephalopathy (PML) is a rare fatal infection caused by John Cunningham virus (JCV) that usually occurs in immunocompromised patients. Since any area of the brain can be involved, PML shows diverse clinical features. The diagnostic criteria of PML are comprised of evidence from clinical, imaging, and virologic studies [1].
PML has no approved treatment except for immune reconstitution. Although in vitro studies and some case reports suggest an anti-JCV property of mefloquine [2-22], the efficacy of mefloquine for JCV is controversial [23,24]. We describe a possible PML case with negative cerebrospinal fluid (CSF) polymerase chain reaction (PCR) for JCV that was successfully treated with mefloquine.
Case Report
A 52-year-old male patient visited the emergency department with a 2-week history of positional vertigo, a 3-day history of tinnitus, ear pressure, and hearing loss in the left ear. He denied other neurologic symptoms. He had a history of coronary stent insertion for myocardial infarction and living-donor kidney transplantation for end-stage renal disease of unknown etiology. He was taking prednisolone 5 mg daily with mycophenolate mofetil 360 mg twice a day.
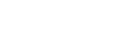
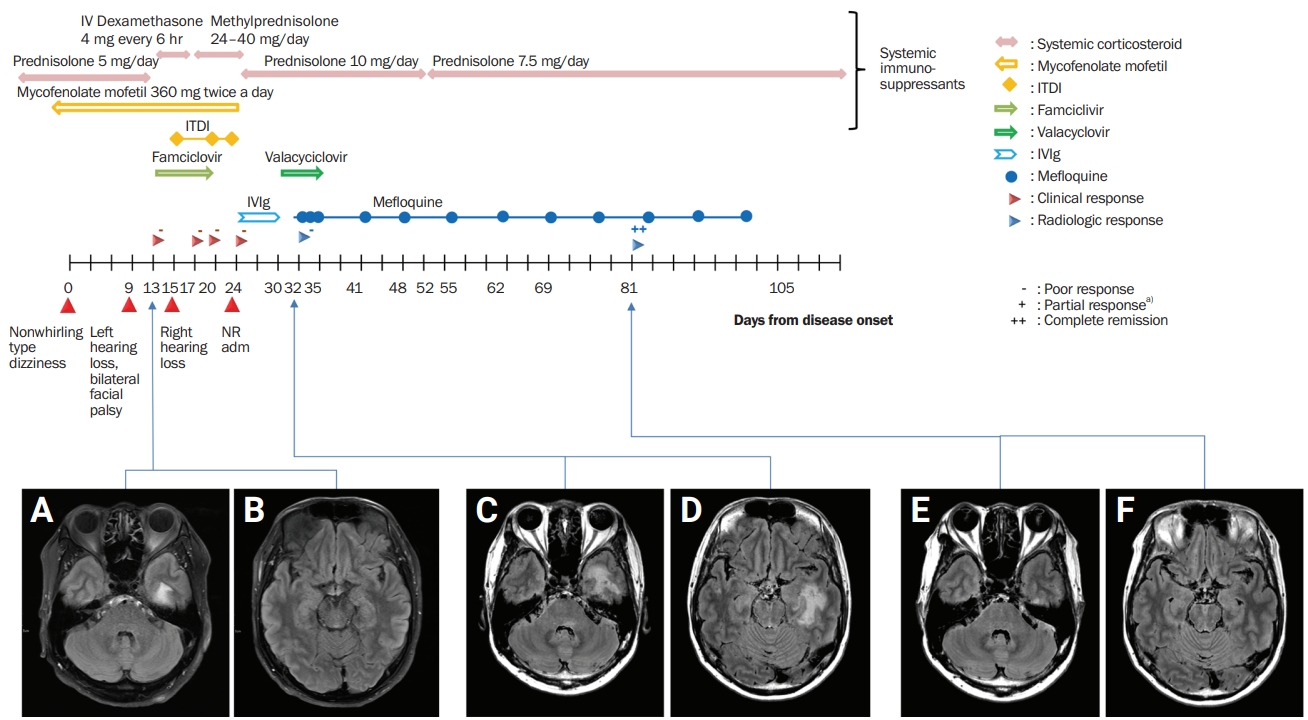
Neurologic examination revealed Weber lateralization to the right side, bilateral nasolabial fold blunting, and truncal ataxia. However, other cranial nerves, motor, sensory, and cerebellar function tests, and the otoscope examination were unremarkable. The initial impression was multiple cranial nerve palsy. Brain magnetic resonance imaging (MRI) revealed bilateral facial nerve enhancement (left > right) and subtle fluid-attenuated inversion recovery (FLAIR) hyperintensity and T1 hypointensity in the left temporal white matter (Figure 1A and B).
He was admitted to the otorhinolaryngology department with the initial impression of Ramsay-Hunt syndrome. The patient received intravenous dexamethasone 4 mg every 6 hours for 4 days, oral methylprednisolone 40 mg for 10 days, and famciclovir 500 mg for 7 days. Intratympanic dexamethasone was administered three times in the left ear and twice in the right ear, but the administration aggravated the patient’s bilateral sensorineural hearing loss.
He was referred to the neurology department and was admitted with the impression of encephalitis of infectious or autoimmune etiology. CSF examination showed marginal pleocytosis (leukocytes, 8 cells/µL; lymphocytes, 75%; others, 25%) with a normal protein level (39 mg/dL) and negative results for the Gram stain, bacterial culture, and cryptococcal antigen (Table 1). Valacyclovir 1,000 mg twice a day for 1 week and intravenous immunoglobulin G (IgG) 2 g/kg over 5 days were prescribed. The corticosteroid dose was tapered to oral prednisolone 10 mg daily. CSF PCR revealed a positive result for Epstein-Barr virus (EBV) and negative results for mycobacteria, cytomegalovirus, herpes simplex virus, varicella zoster virus (VZV), and JCV. The result of serum JCV PCR was positive. EBV viral capsid antigen (VCA) IgG was positive, but EBV VCA IgM was negative. Early antigen and EBV nuclear antigen tests were not conducted (Table 1).
After 2 weeks of antiviral treatment, follow-up brain MRI showed FLAIR hyperintensity and T1 hypointensity in the subcortical white matter of the left temporal lobe and dorsal pons (Figure 1C and D). The imaging findings suggested lymphoproliferative disease or PML. Whole-body positron emission tomography was performed to rule out the possibility of lymphoproliferative disease and revealed no abnormal hypermetabolism, which would suggest malignancy. In the meantime, an initial workup that included ganglioside antibodies, antinuclear antibody, antineutrophil cytoplasmic antibody, angiotensin-converting enzyme level, aquaporin-4 IgG, myelin oligodendrocyte glycoprotein IgG, vitamin B12, and folate level showed that these levels were normal. He was diagnosed with possible PML. Because of the patient’s poor response to the antiviral agent and the results of his extensive diagnostic workup, we excluded other differential diagnoses, including VZV leukoencephalopathy, central nervous system (CNS) vasculitis, and lymphoproliferative diseases. Nevertheless, the corticosteroid was tapered to prednisolone 10 mg equivalent, brain MRI showed increased extent of the FLAIR hyperintensity lesion, and pure-tone audiometry (PTA) showed progressive bilateral sensorineural hearing loss. Since steroid tapering was not sufficient to halt disease progression, mefloquine 250 mg/day for 3 days was introduced and maintained at 250 mg every week. After mefloquine treatment, his neurologic deterioration stopped, and no other focal neurologic deficit, other than the presenting sensorineural hearing loss, appeared. In the 6-week follow-up MRI, previous white matter lesions were markedly decreased, and serum JCV PCR was negatively reversed (Figure 1E and F). Initially, we planned maintenance treatment with mefloquine to continue until radiologic remission or confirmed recovery of hearing. However, the maintenance therapy of mefloquine 250 mg/week was administered for only 8 weeks due to the patient’s refusal. At his nadir, he was only able to follow simple commands, but after treatment, his sensory aphasia improved to almost normal and his cognitive function improved to independent activities of daily living. A change in his hearing deficit, however, was not assessed due to the patient’s refusal for PTA follow-up.
Discussion
PML is prevalent in immunocompromised patients. Although JCV infects more than 50% of the adult population, its replication is suppressed by antigen-specific T cells in immune-competent individuals [1]. In an immune-compromised subject, however, JCV can replicate in oligodendrocytes and astrocytes causing lytic necrosis, which is a key factor in the pathophysiology of PML [25].
No single criterion has been established for the diagnosis of PML. The American Academy of Neurology suggests that clinicians diagnose PML based on evidence from clinical, neuroimaging, and virologic studies [1]. Given these criteria, the definite or probable PML case requires positive CSF JCV PCR or histopathologic evidence in brain biopsy. However, several reports describe negative CSF JCV PCR cases that were finally diagnosed as PML [3,22,26-34]. In a search on PubMed, at least 11 case reports published in English were available, and each case was biopsy-proven [3,22,26-34] (Table 2). Some new diagnostic criteria of PML have been proposed to overcome this limitation [35]. Our case had clinical and imaging features supporting PML and was categorized as possible PML. Other possibilities, like CNS vasculitis and VZV leukoencephalopathy, were excluded through an extensive diagnostic workup. A brain biopsy was required to confirm the diagnosis of PML; nonetheless, brain biopsy was spared in this patient due to its invasiveness and empirically treated as PML.
The only approved treatment of PML is immune reconstruction. This approach is based on the fact that PML is one of opportunity infections. The removal of immunosuppressants in treatment-related PML and antiretroviral therapy in human immunodeficiency virus-associated PML are good examples. Treating PML with immune checkpoint inhibitor is also a similar strategy [36].
Other strategies are based upon in vitro studies. Mirtazapine or atypical antipsychotics were expected to inhibit viral entry into cells blocking 5HT2A receptors, which is a cellular receptor for JCV. For these medications to be validated as treatment options for PML, their toxicity should be tolerable in the therapeutic range, and the drugs should be delivered to the CNS. In vitro studies suggest that mefloquine not only has an anti-JCV property by inhibiting viral DNA replication but also sufficiently penetrates the blood brain barrier [2]. Moreover, these in vitro studies are supported by several case reports of PML successfully treated with mefloquine [3-22,37]. In PubMed, at least 21 case reports published in English were available, and these cases even included treatment without additional immune reconstitution therapy [3-22,37] (Table 3). Some clinical studies failed to show the clinical efficacy of mefloquine [23], but some points must be considered. A large clinical trial of PML is difficult due to its rarity. In addition, it seems that ABCB1/MDR1 gene polymorphism has an important role in pharmacokinetics and efficacy [24], contributing to the negative results of the trial [23].
In the present case, although the virologic evidence was not fulfilled, clinical and imaging findings led to the impression of PML. Immunosuppressants were tapered but failed to halt the disease progression, and mefloquine treatment was administered.
According to pharmacokinetic studies, the biologic half-life of mycophenolate, prednisolone/methylprednisolone, and intravenous Ig were reported as 9 to 17 hours, 12 to 36 hours, and 14 to 35 days, respectively [38-40]. Since 4 half-lives is usually considered sufficient time to reach the steady state, it seems that the half-lives of the corticosteroid and mycophenolate mofetil are too short and the half-life of intravenous Ig is too long to explain our patient’s delayed and prolonged treatment response 1 month after onset. Therefore, with all these confounding factors including other immune-related medication changes, it is reasonable to conclude that mefloquine led to improvement of the PML.
Therefore, physicians can learn two points from this case. A negative CSF JCV PCR does not always rule out PML. Moreover, when PML is clinically highly suspicious and brain biopsy is difficult, a mefloquine trial can be considered as an option.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






