A case of invasive Klebsiella pneumoniae syndrome with ventriculitis
Article information

Dear Editor,
Klebsiella pneumoniae is a member of the Enterobacteriaceae family and an established cause of urinary tract/hepatobiliary infections and osteomyelitis, especially in alcoholics and diabetic patients [1]. In the 1980s, a new hypervirulent variant of K. pneumoniae was reported; it causes lung, prostate, and soft tissue abscesses and is associated with metastatic complications such as endophthalmitis/uveitis and central nervous system infection [1,2]. The mortality rate ranges from 3% to 42% [3]. We present a case of ventriculitis and multiple metastatic infections caused by K. pneumoniae in a patient with chronic alcoholism and uncontrolled diabetes who survived after appropriate antimicrobial and surgical treatment. Informed consent was provided by the patient and his family for this report.
A 60-year-old male was admitted to the department of internal medicine with fever, general weakness, and dyspnea that presented 4 days prior to admission. Levofloxacin (750 mg daily) was initially administered for treatment of suspected pneumonia. He had hypertension, diabetes, and a 30-year history of daily alcohol consumption. The patient became drowsy and confused on the 2nd day of admission and was transferred to the department of neurology. His vital signs were stable except for fever of 38.9ºC. Neurological examination showed impaired consciousness (Glasgow Coma Score E3 V2 M4) and nuchal stiffness. White blood cell (WBC) count was 12.64 × 103/μL with an elevated neutrophil percentage of 82.8%. The levels of C-reactive protein, procalcitonin, glucose, and hemoglobin A1c were 45.88 mg/dL, 0.65 ng/mL, 393 mg/dL, and 7.6%, respectively. Brain diffusion-weighted magnetic resonance imaging revealed septic encephalitis with pyoventriculitis (Figure 1A). Contrast-enhanced chest and abdominal computed tomography (CT) revealed septic emboli in bilateral lungs (Figure 1B) and abscesses in the liver (Figure 1C) and prostate (Figure 1D). On cerebrospinal fluid (CSF) examination, the gross appearance of CSF was clear with a straw-like color. WBC count and the levels of glucose and protein were 18,500/μL (polymorphonuclear leukocytes, 95%), 6 mg/dL, and 344.7 mg/dL, respectively. We administered intravenous ceftriaxone (2 g twice daily), ampicillin (2 g every 4 hours), vancomycin (1 g twice daily), and metronidazole (500 mg thrice daily) empirically.
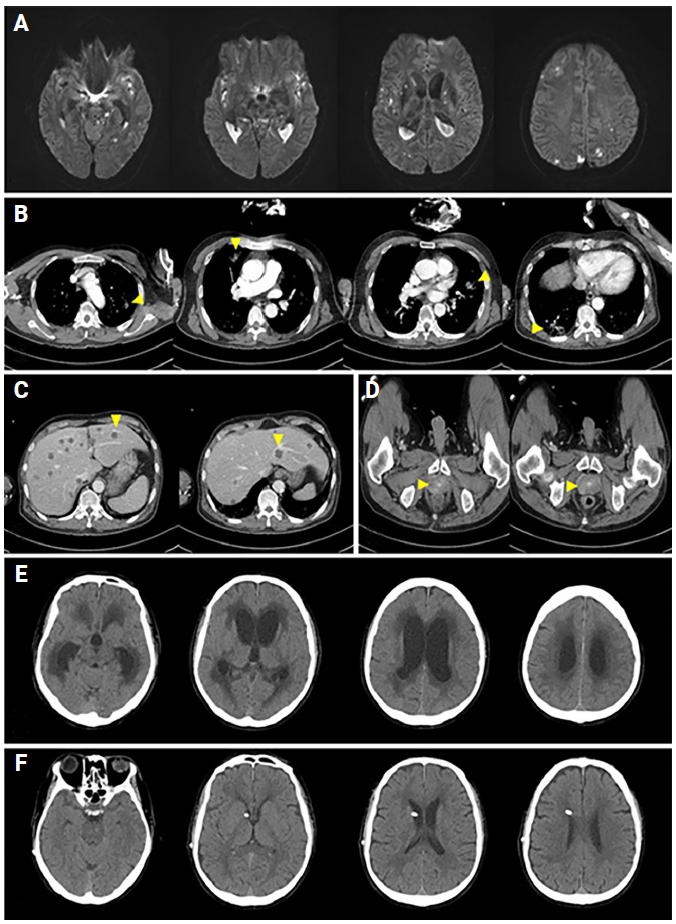
Initial brain magnetic resonance imaging, contrast-enhanced CT of the chest and abdomen, and follow-up brain CT before and after VP shunt insertion
(A) Brain diffusion-weighted magnetic resonance imaging shows diffusion restriction in both lateral ventricles and multifocal foci, which are indicative of septic encephalitis with pyoventriculitis. (B) Contrast-enhanced CT of the chest shows numerous, variably sized nodules and ill-defined peribronchial consolidation (arrowheads) in both lung fields. (C) Contrast-enhanced CT of the abdomen shows multiple small hepatic cysts (arrowheads) suggestive of necrotizing solid lesions. (D) Contrast-enhanced CT of the pelvis shows prominent enhancement in the prostate. (E) Brain CT before VP shunt insertion shows hydrocephalus of the lateral and 3rd ventricles with interstitial edema. (F) Brain CT shows decreased dilatation of the lateral and 3rd ventricles after VP shunt operation.
CT, computed tomography; VP, ventriculoperitoneal.
On day 4 of admission, two sets of peripheral blood cultures grew K. pneumoniae, which was sensitive to all tested antibiotics, including ciprofloxacin, except ampicillin. Ceftriaxone (2 g twice daily) and ciprofloxacin (400 mg twice daily) were used according to the result of antimicrobial sensitivity test. Uncontrolled diabetes mellitus was treated using insulin. Endophthalmitis was observed in the left eye on the same day. CSF culture grew K. pneumoniae having antibiotic susceptibility similar to that obtained from the first blood culture. On day 21 of admission, ciprofloxacin was discontinued. After treatment, the patient gradually became alert and oriented. The follow-up CSF examinations performed every week showed gradual decrease in WBC count and protein and increase in glucose. No bacteria were grown on blood and CSF cultures. The count of WBC and the levels of glucose and protein on day 41 were 9/μL, 43 mg/dL, and 105.6 mg/dL, respectively. The level of protein was 53.6 mg/dL on day 55. Ceftriaxone was used until day 41 and changed to oral levofloxacin (750 mg daily).
On day 42 of admission, the patient again became drowsy and confused with aphasia and urinary incontinence. A follow-up brain CT showed hydrocephalus involving both lateral and 3rd ventricles, with interstitial edema (Figure 1E). Since intermittent CSF drainage had failed to improve his consciousness, we consulted the department of neurosurgery, which performed ventriculoperitoneal (VP) shunt operation. After the surgery, he became alert and oriented. Follow-up brain CT showed normalization of the size of the lateral and 3rd ventricles (Figure 1F). The patient underwent rehabilitation and was discharged without focal neurologic deficit. Despite administration of topical antibiotics, antiglaucoma medication, and atropine, he became blind in his left eye as a result of endophthalmitis.
Patients with bacterial ventriculitis are usually treated with intraventricular lavage in combination with intravenous and intraventricular antibiotics [4]; however, the prognosis is poor [1]. Hydrocephalus, which is a complication of pyogenic ventriculitis, can lead to aggravation of impaired mental and neurological status. In a previous study, patients with pyoventriculitis who developed hydrocephalus received a VP shunt after the infection was controlled; none developed reinfection or peritonitis after surgery [4]. Although the mortality rate of K. pneumoniae meningitis ranges from 38% to 91% [5], appropriate antimicrobial therapy with VP shunt operation can lead to good outcomes [4]. Clinicians should be aware of invasive Klebsiella syndrome because of its rapid progression and high mortality. High clinical suspicion, especially in alcoholic patients or those with uncontrolled diabetes; timely investigation for other metastatic infections; and use of appropriate antibiotics are essential to improve patient outcomes. This case shows that rapid diagnosis and treatment of invasive Klebsiella syndrome of the central nervous system are crucial for patient survival without significant sequelae. This case also shows that VP shunt operation should be actively considered for patients who develop severe hydrocephalus.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Conceptualization, Data curation, Formal analysis, Visualization, Resources: Youn M, Lee JJ; Investigation, Software, Supervision, Validation: Lee JJ; Methodology, Project administration: all authors; Writing–original draft: Youn M, Lee JJ; Writing–review & editing: all authors